


A 6-year-old girl who loves gymnastics and arts and crafts has become the first person in South Carolina to get a successful partial heart transplant. The heart team at the MUSC Shawn Jenkins Children’s Hospital, one of the top-ranked programs in the country, performed the procedure on Elaine Smith of Conway.
“We are one of the few centers in the country that offer this,” said pediatric cardiothoracic surgeon Minoo Kavarana, M.D. “So far, there have been fewer than 50 partial heart transplants done in the country.”
Elaine’s mother, Bethany Smith, said she and her husband, Josh, were cautious when they first heard about the operation from a cardiologist.
“The doctor told us that there was a new procedure and Elaine would be the perfect candidate. She said, ‘It's called a partial heart transplant or living tissue transplant.’ And so I was like, ‘I'm sorry, you said what now? A partial heart transplant – that's not even a thing, is it?’ And she said, ‘It sounds like something made up, but it is a new procedure that we have.’”
What a partial heart transplant is
It’s easy to see why the Smiths were thrown off. The procedure isn’t well-known and has only been around for about four years.
But it’s familiar to heart specialists at the MUSC Shawn Jenkins Children’s Hospital, where the concept originated. Pediatric cardiac surgeon Konrad Rajab, M.D., was working there in 2022 when he came up with the idea of transplanting living heart valves from human donors into children who would otherwise get animal, cadaver or mechanical valves that would need to be replaced as they grew up.
Rajab partnered with surgeons at Duke University on his concept. MUSC and Duke performed the first preclinical transplants on porcine models. The first human partial heart transplant in the country was performed at Duke four years ago.
As the procedure has become better established, data is starting to come in. Researchers report in the Journal of the American Medical Association that among 19 people who had partial heart transplants and took medication to keep their bodies from rejecting the transplants, all of the valves were working and grew over time. “Partial heart transplant appears to be a safe and feasible procedure that enables valve growth,” they concluded.
Kavarana and his team started looking for appropriate candidates for a partial heart transplant at the MUSC Shawn Jenkins Children’s Hospital and listing them with Surge Ingenuity, an FDA-approved agency that supports this procedure.
The right candidate
The right candidate turned out to be Elaine. The Horry County girl was diagnosed with heart problems in utero and referred to MUSC Children’s Health. It has a Maternal Fetal Medicine program for high-risk pregnancies and cardiologists specializing in caring for babies and children with heart trouble.
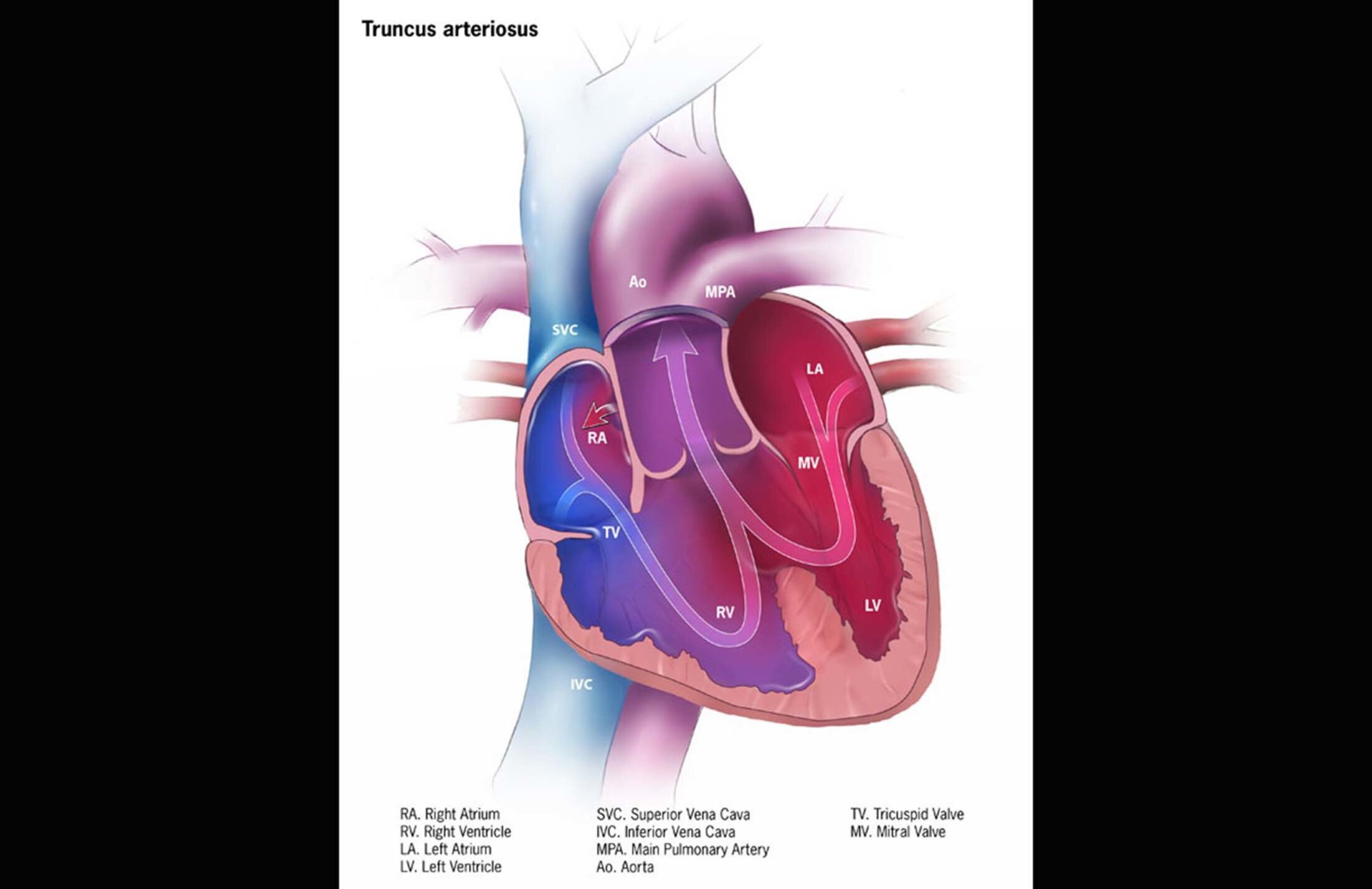
Elaine had a rare heart defect called truncus arteriosus with an interrupted aortic arch. Instead of having two arteries carrying blood away from the heart, she had one big one known as the truncus. And it was leaking. She also had a hole in the wall between her heart’s two pumping chambers.
So Elaine had lifesaving open heart surgery when she was just 6 days old at the MUSC Shawn Jenkins Children’s Hospital. The procedure included implanting an artificial tube and valve to link her right ventricle to the arteries going to her lungs and repairing her outflow valve.
The operation was a success, but the implants would stay the same size while Elaine continued to grow. That meant she’d need repeated operations in the future to replace them. And the repaired valve, which continued to leak, would likely need to be replaced one day as well.
Her parents knew that day might be near when they noticed changes in Elaine last November. “She was just slowing down,” her mom said. “She just wasn't keeping up with her cousins and her friends at gymnastics, her friends at school, and she had to take breaks, and when she was home, she would just lie on the couch and go straight to sleep.”

At Elaine’s six-month cardiology checkup, tests showed her heart wasn’t pumping properly anymore. That’s when her cardiologist told her parents about the possibility of a partial heart transplant. They met with Kavarana to discuss the potential risks and benefits.
“After I laid out all potential options available for Elaine, I let her parents make their own decision. It's what I like to call shared decision-making,” the surgeon said.
That decision wasn’t easy for a couple of reasons. First, there isn’t any long-term data yet on partial heart transplants, although early results are strong. Second, Elaine would temporarily have to take medication to suppress her immune system, which would make her more susceptible to infections and other health issues.
But Smith said, for her, the upsides outweighed those concerns. She and her husband liked the fact that living donor tissue, unlike artificial material, could grow with Elaine.
“Had we not gone with the partial heart transplant, the only other solution would have been to put her on a mechanical valve, which would've put her on blood thinners for the rest of her life. Or she would get a cryopreserved (cold) homograft (human valve) that typically malfunctions in five to 10 years,” Smith said.
“Either of these options would double how many surgeries she would need in the long run. And of course, because she's a female, being on a blood thinner can also interfere with the chances of her having children one day. I didn’t want to take that away from her.”
So the decision was made. Physician assistant Eleta Donelan, who specializes in pediatric cardiac surgery, got Elaine listed for transplants to replace her aortic and pulmonary valves.
The operation
When donor valves became available, it was time for the operation. It took about nine hours as Kavarana worked with pediatric cardiac surgery fellow Kenichi Okamura, M.D., and the rest of their team to perform the procedure.


While they replaced the two heart valves that weren’t working, they also repaired an abnormal left coronary artery. That significantly increased the complexity and risk of the operation.
The procedure called for a large team of care providers. Donelan described the range of people who helped make it possible. “Everyone involved with taking care of Elaine, including our ICU cardiologists and intensivists that worked to get her extubated so quickly and up and out of bed and moving so we could get her tubes out, was essential,” she said.

“Our pediatric advanced cardiac therapies team helped us find the perfect candidate in Elaine. Our nurses were critical, too. So many people were involved in making sure she was able to go home in seven days, which was a huge feat.”
Hopes for Elaine’s future
Kavarana hopes another feat will follow. “My hope for Elaine is that she comes off the immunosuppressant,” he said.
“I've suggested that she stay on it for nine to 12 months and then she comes down to a low dose. I think if she stays on half of one of the three medications for an extended period of time, the toxic side effects will be very minimal, and it can still protect her from rejection.

Elaine’s parents are looking to the future as well. “I hope that she grows healthy and happy, but most importantly, knowing there is nothing wrong with her. She is beautiful. She is strong. She is smart. Because to me, the biggest thing is having confidence in yourself,” her mom said.
“With her having to go through these surgeries and having all these scars, girls get self-conscious. I want her to be proud of her scars. I want her to be proud of who she is and what she's overcome and hold her head high. And I hope she does that from this day forward because she's done it since birth."

Minoo Naozer Kavarana, M.D., FACS
Minoo Kavarana, M.D., is a pediatric cardiothoracic surgeon who joined the department in 2010. In 2023, he was appointed the inaugural division chief of the newly created Division of Cardiothoracic Surgery in the Department of Surgery. Dr. Kavarana also serves in MUSC Health as Co-Director, Pediatric and Congenital Heart Center, and is the Surgical Director of the Pediatric Heart Transplantation and Mechanical Support.
Dr. Kavarana's clinical expertise include neonatal and infant heart surgery, adult congenital heart surgery, heart and lung transplant and mechanical circulatory support. He graduated from medical school in India in 1994. Following this he received post-graduate training in general surgery at New York Medical College, where he spent a year at Columbia University, New York as a heart transplant and ventricular assist device post-doctorate fellow. He then received cardiothoracic surgery training at the Jewish Hospital, University of Louisville, Kentucky where they implanted the first implantable total artificial heart. During this time, he developed a deep clinical and research interest in pediatric cardiac disease, pediatric cardiac assist and thoracic organ transplantation. Following this he completed a congenital heart surgery fellowship at the University of Michigan in Ann Arbor with Dr. Edward L. Bove.
In 2010, Dr. Kavarana joined MUSC in the division of cardiothoracic surgery. Dr. Kavarana's clinical interests include neonatal and infant heart surgery, adult congenital heart surgery, heart and lung transplant and mechanical circulatory support.



